Essential Requirements for the Parameterization of Food Waste in Hospitals

This research explores the topic of food waste from the economic perspective to provide a framework for improving both cost and process efficiency. The methodology is based on an exploratory multiple-case study involving three Swiss hospitals.
Essential Requirements for the Parameterization of Food Waste in Hospitals
Gabriela Züger1 and Franziska Honegger2
Abstract
Food waste in private households, as well as in the food production industry is becoming a more important topic these days. In addition, food waste in hospitals is an emerging topic primarily because hospitals are now being forced to enhance process efficiency and cost transparency in the face of more stringent economic circumstances such as budget cuts and austerity measures. So far, the body of literature dealing with the food waste issue in hospitals focuses mainly on the causes and effects of malnutrition. This research sets out to explore the topic of food waste from the economic perspective in order to provide a framework for improving both cost and process efficiency. This research focusses on the process section of the plated food leaving the kitchen, being delivered to the patient and returning to the dishwashing area as food waste. The methodology is based on an exploratory multiple-case study involving three Swiss hospitals conducted via structured observation, document review and unstandardized interviews. Results show that the parameters most strongly influencing food waste are related to the service such as meal ordering by patients, delivery of the food and the collection of the trays after consumption. The different interfaces between the different tasks, as well as between the different staff categories are important for the prevention or at least reduction of food waste during the whole food service process. Well working logistic processes are a precondition for good food service quality. Results also provide data on different food waste components such as the proportion of bread wasted after breakfast. For example, from the bread distributed on patient trays on average 5% returned untouched, 49% partly eaten and 46% eaten. The results also showed that besides bread, the main food components resulting in waste are salad and dessert.
Keywords: Food Waste, Healthcare, Hospital, Process, Facility Management
Introduction & Background
The healthcare system in Switzerland is one of the most expensive in the world and the costs are increasing every year. For that reason, on the first of January 2012, Switzerland introduced a new remuneration system called Swiss Diagnosis Related Group (Swiss DRG). This funds the stationary hospitals’ activities with lump sum compensation payments. One of the reasons for the implementation of Swiss DRG is to gain more transparency and comparability in order to enhance efficiency (SwissDRG, 2013a, 2013b). This demand for transparency is not only being made of the core activities of the hospitals but also of many support processes. According to the European Committee for Standardisation, support processes can be collectively referred to as facility management (FM), which is defined as the “integration of processes within an organisation to maintain and develop the agreed services which support and improve the effectiveness of its primary activities” (CEN, 2006, p. 5). The European FM understanding explicitly includes both hard and soft FM services. In line with the European FM understanding food services, being a support process, have an important role in the core activities of a hospital because patient satisfaction is very much influenced by the quality of the food provided. (von Eiff, 2012).
It is interesting to note that most research projects on hospital food focus on the causes and effects of patient malnutrition and that, according to the literature the measurement of food waste has been a side effect of this research rather than a research area of its own (Barton, Beigg, MacDonald, & Allison, 2000; Dupertuis et al., 2003; Edwards & Nash, 1999; Sonnino & McWilliam, 2011). However, the work done by Williams and Walton (2011) shows that, despite having been treated as a side issue over the last 50 years, food waste has been and still is a topic worthy of examination.
Data on food waste in hospitals is scarce. Barton et al. (2000), report that 30% of the plated food for patients is wasted and 11% of the prepared trays are returned untouched. Almdal, Viggers, Beck, and Jensen (2003) went into more detail, they found that 30 -40% of the food produced for patients was returned uneaten, 40 -45% was eaten and for the last 20 -30%, it was not clear what had happened to it. These figures show that there is a lot of room for improvement in hospital food services to reduce the amount of waste.
Taking the above data into account, it is clear that despite the fact that it has been the focus of most research to date, patient malnutrition is not the only problem that hospitals face. The provision of food in hospitals is strongly affected by cultural factors and the cost of providing food. The FM which is responsible for providing food to patients is concerned primarily by food costs, first by costs of production and delivery from and to the wards and secondly by disposal costs.
To increase transparency within food service processes, a benchmarking platform for Swiss hospital catering has been developed (Hofer, Honegger, & Züger, 2013). As the costs of Meals per Patient per Day could not be drawn out of the existing cost structures, a specific method was established. During the development of this, awareness of the impact of food waste on the process of food provision arose and has been continuingly developed. Based on this, actions were taken to measure food waste in two different ways: The number of trays which came back untouched from the patients to be thrown away and the weight of returned food scrapings were recorded separately. To calculate the value of food wasted, the weight of food scrapings was then multiplied by the average cost of goods used in the preparation of the food.
Results showed that 15% of all the trays delivered to the wards for the patients were returned untouched to the dishwashing area, and that the value of the food wasted totalled 30% of the value of ingredients used to prepare it. These findings support the results of Barton et al. (2000), mentioned above.
It was beyond the scope of the project to check if all the delivered meals to the wards had been eaten by patients or if they were consumed by third parties, such as staff. These results highlight the importance of examining the reasons for food waste in food service processes in hospitals more closely. This study will address this research gap.
Identifying Essential Requirements for the parameterization of Food Waste
Methodology
Research question
Based on the situation described above, the leading research question was: What parameters are important for the improvement of food service processes in Swiss hospitals, with a focus on food waste?
The aim of this research was to investigate the current catering processes in Swiss hospitals in order to discover which factors influence food waste. These factors serve as indicators on which improvements within the processes can be based. As such, they provide a starting point for further research projects, as stated in the outlook section of this paper.
Qualitative case study design
To achieve the above mentioned aims in the context of having unknown factors, a multiple case study was conducted using a qualitative, exploratory approach. According to Robson (2002, p.178) as cited in Saunders, Lewis, and Thornhill (2009, pp. 145-146) a case study is defined as: “a strategy for doing research which involves an empirical investigation of a particular contemporary phenomenon within its real life context using multiple sources of evidence”.
The topic of the multiple case study was food services in each of the three hospitals. The idea was to discover if new insights from one case could be found in other cases as well. The focus was on the part of the process when the plated food leaves the kitchen, is delivered to the patient and returned to the dishwashing area as food waste. These limitations needed to be made, due to the available research resources. Initially three different hospitals which use the cook & serve system of food production were chosen. Based on the research question, the different actions in these settings were described. Furthermore, the collected data was then analysed in a descriptive way.
Case access / sampling
Based on Flick (2010, p. 125) the sampling cannot be taken out of the context in which it is used. Therefore, the three hospitals were selected based on the following four criteria. The hospitals are located in the German speaking part of Switzerland, they are publicly owned, they are acute-care hospitals within the hospital category “Allgemeinspital Zentrumsversorgung Niveau 2” (Bundesamt für Gesundheit BAG, 2013). Also, they all provide food using the cook & serve system. According to von Eiff (2012, p. 78) almost 95% of the hospitals in Switzerland use the cook & serve system. This was followed by a purposive sampling which is used when working with a very small sample (Saunders et al., 2009).Table 1 provides an overview of the key parameters of the three hospitals.
Table 1. Key Parameters of Sample Hospitals (all acute-care)
| | Hospital 1 | Hospital 2 | Hospital 3 |
| Number of beds | 377 | 540 | 684 |
| Inpatients | 18,406 | 26,611 | 28,155 |
| Inpatient days | 106,744 | 191,405 | 222,008 |
| Number of staff (FTE) | 1,325 | 3,693 | 3,847 |
| Number of staff (headcount) | 1,940 | 4,476 | 4,841 |
Data collection and analysis
In line with qualitative research design and exploratory multiple case study design, data collection was done using the following methods. Data collection was conducted over a period of five days, covering the times of the three main meals, in each of the three hospitals. Structured observations (focusing on the logistics, the service on the wards and food waste on the trays) with additional measurements of transport time as well as photographs of the trays with the food waste; unstandardized interviews (staff members responsible for food provision) and document research (mainly customer and staff information related to food provision). The different types of data provided a detailed picture of the different cases from various perspectives. Informant verification was conducted between the observations and the interviews.
The data from the structured observations, the unstandardized interviews and the document research were put together into a data matrix, which was then analysed in a descriptive way. The measured transport times were compared with the specified conditions. The photos were not analysed in great detail as is the norm for visual material. The information from the photos of food waste on the trays was filled into an analysis guideline, based on the different menu and tray components. Out of the transport times and the food waste data, figures of qualitative value were created. In Table 2 an overview of weekly average of the number of trays per meals, which were calculated using the photos, is given. Based on the three cases a deduced version of the different results was generated.
Table 2. Number of Trays Per Meal (week average)
| | Hospital 1 | Hospital 2 | Hospital 3 | Deduced hospital |
| Breakfast | 17.33 | 16.00 | 15.33 | 16.22 |
| Lunch | 7.50 | 12.50 | 14.00 | 12.33 |
| Dinner | 6.00 | 14.00 | 16.75 | 12.25 |
Findings
The findings of the data analysis are divided into four different sections. First, the parameters on food waste during the process of food delivery are focused on. Then a closer look is taken at transport times, followed by an examination of the food waste components based on the photos. Finally the status of the trays at collection time is considered. All figures are based on average numbers of trays per meal of the three investigated hospitals. This combined knowledge can form the basis for improvements to food service processes for future projects on food waste.
Food waste parameters
The most important parameter for food waste in the food service process is the various interfaces between staff categories, as well as the various tasks conducted by the staff. These are very important in order to have the highest possible service quality with the lowest possible amount of food waste. In general, food waste cannot be influenced anymore after consumption. During the ordering and service tasks food waste can be greatly influenced. For this service to work well, smooth logistic processes with in-time delivery are required as a precondition. During ordering, patients are asked which menu item and which portion size they would prefer. This helps to prevent food waste and gives autonomy to the patients. The whole ordering process step is time consuming for staff. For the patients it is a nice change in the daily routine. When the ordering is being done, the mental and physical condition of each patient needs to be taken into consideration. After the nutritional counselling has taken over the responsibility, no changes in the ordering system can be done by the nurses or the hotel service team who are normally in charge of the ordering process. Due to a range of medical considerations, patients can require special diets which are physician-directed. Occurring within the above mentioned parameters, ordering has a high impact on food waste. If a mistake occurs during this stage, it cannot be rectified, and food will almost certainly be wasted.
During the service it is important that patients are positioned correctly before the food trolley is delivered to the ward so that patients can immediately start to eat. When the trays are distributed to the patients, they get help to prepare to eat their meal as well as to eat it, if needed. Patients have a minimum of 30 minutes time to eat each meal, with no interruptions taking place. This helps to provide the best food quality possible to the patient, as well as to assure they have a good food intake to prevent malnutrition.
At first glance, logistics do not seem to have a high impact on food waste, but as it is an extension of the kitchen team to their customers (the patients) it has an essential role. During the logistics of moving the trolleys from the wards to the dish-washing area, food waste cannot be influenced anymore. The task related to food waste in this process step is to bring all the food waste to the place where the correct disposal takes place.
Overall, many different parameters are involved in the prevention and encourage of food waste in the process of food services. They are shown in a short summary in the Table 3:
Table 3. Parameters on Food Waste
| Generic | Task and staff category interfaces |
| Ordering | Nutritional counselling, no changes possible by nurse Mental and physical condition of patient Time intensive Asking menu and size Special diet physician-directed |
| Service | Patient have minimum 30 minutes time to eat Give help to patients to prepare to eat the meal or/and to eat Patient positioning is needed No interruptions during consumption |
| Logistics | In time delivery |
Transport times of the food trolleys
Due to the fact that the trolleys need to be delivered on time to the wards for patient safety, the transport times of the plated food is looked at in more detail. Each of the three hospitals has a different logistics concept (automatic transport system, manned logistic system, manned logistic system with logistic vehicle). These depend on the layout of the hospital as well as on how many buildings need to be delivered to.
As shown in Error! Reference source not found., all the food trolleys were either delivered prematurely or in time. No trolleys arrived at the target areas late. In addition, there are no big differences between the three different logistics systems.
Figure 1. Food trolley delivery time
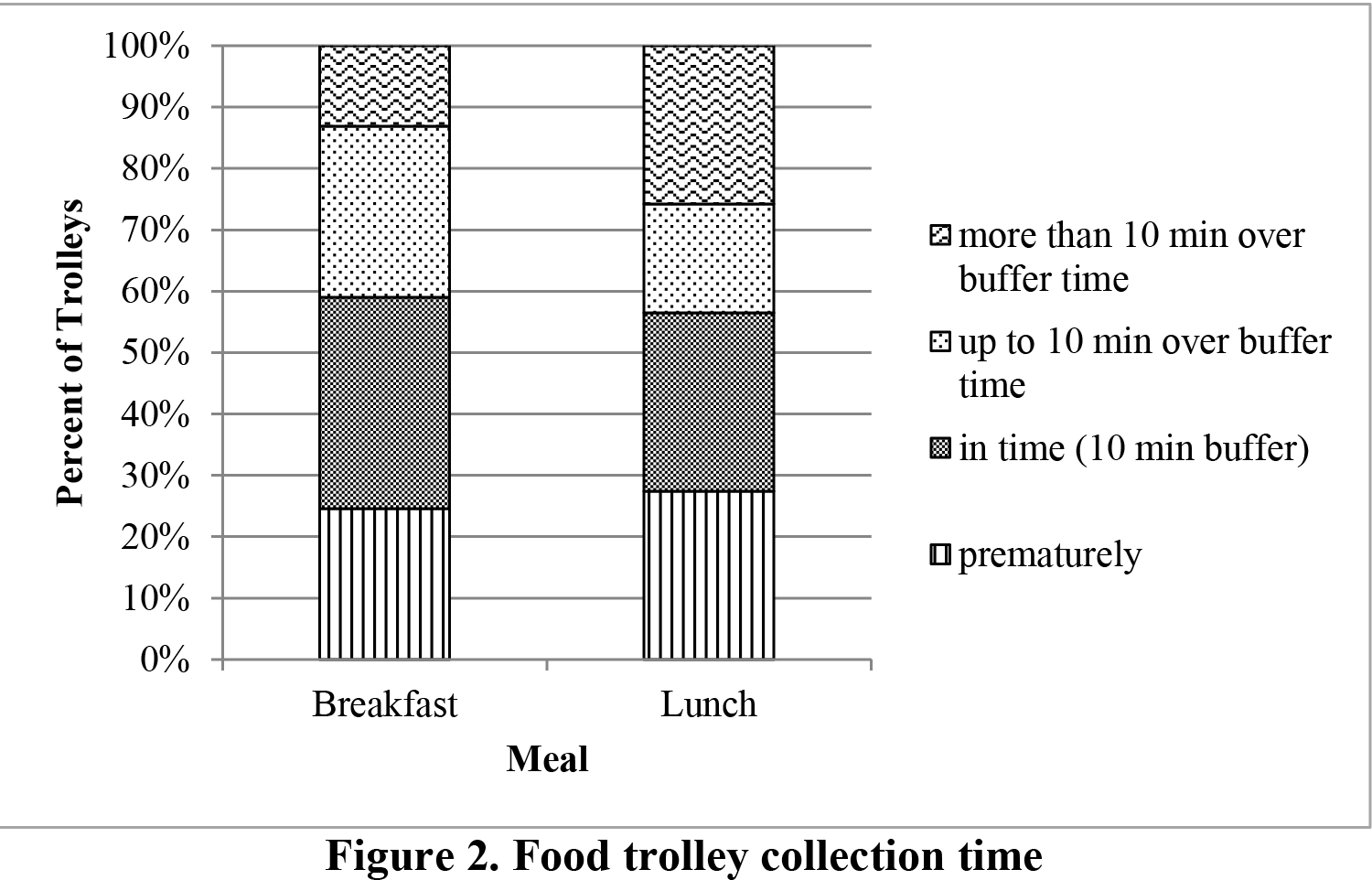
When the trays are placed in the trolleys after consumption, the trolleys need to be brought back to the kitchen for dishwashing and disposal of food waste. During data collection at breakfast in one hospital a technical problem occurred. Therefore, these results cannot be taken into consideration. As shown in Error! Reference source not found., for breakfast almost 60% of the trolleys are collected prematurely and in time, 40% are collected too late. Around 55% of the trolleys are collected prematurely and in time at lunch, 45% are collected too late. Various reasons could be observed for the large differences between the delivery and the collection times, the most common being that the trolleys are moved to the collection area too late. In the three hospitals on most wards the nursing department was responsible for this as well as for the service tasks. This means that the responsibility is leaving the field of authority of the FM. Another reason for the difference is that the delivery is more important than the collection even for the logistics team. Due to the fact that after consumption no influence on the amount of food waste is possible, this is not as serious as missing the right delivery time.
Food waste components
As mentioned above, it was calculated that the value of the food wasted totalled 30% of the value of ingredients used to prepare it. To find out what the 30% of the total food value wasted was made up of, photos are taken when the trays are leaving the patient room and analysed to discover how much of the different components were left uneaten. The following factors were not taken into account in the displayed figures 3 to 5: portion size, menu, as well as the mental and physical condition of the patients.
However, this data was compiled using qualitative methods. Also, only single wards of hospitals were examined at different meal times, so a valuable picture of the overall food waste situation in hospitals is not provided. Nevertheless, these results give additional insights into what the food waste consists of. In order to present these insights, food waste per meal needed to be segmented. This was done on the basis of the meals’ main components and with regard to their costs. This segmentation and also quantification of the relevant components is important to this research because it enables future research to link food waste with costs. The components of the food waste for breakfast are shown in Error! Reference source not found..
Figure 3. Food waste components breakfast
Bread is one of the components which is wasted the most, on around 30% of the trays half of the given portion is left uneaten. In addition, on more than 10% of the trays a quarter of the bread portion is left uneaten. For jam and butter, a bit more than 10% of the portions remain untouched. The fact that half of the jam and butter is uneaten cannot be changed, because the portion size is given with the available packaged portion size. It is interesting to see that all the yoghurt is eaten when it is ordered, this is most likely due to the fact that it is an additional component to the standard tray that needs to be ordered on specific request. Mostly it is used for medical reasons such as to assist with the swallowing of tablets. More than 40% of the fruit are not touched. From observation it was obvious that the type and maturity of fruit was often a problem for patients lying in bed. It would be a good idea to deliver freshly made fruit salad or slices of fruit, as they are easier to eat when lying in bed. More than 30% of cheese portions are not touched. A possible reason is the packaging, which is hard to open. Almost 20% of the special components (birchermüesli, omelettes) are not touched.
Figure 4. Food waste components lunch
As shown in Error! Reference source not found., the main food waste components for lunch are salad and dessert. Salad and dessert is either eaten or left completely untouched. The amount
of food waste from the soup cannot be estimated, because it was often either spilled on the trays or the amount was not clear in the photographs and could not be estimated. Protein, vegetables and carbohydrates are eaten, but sometimes not the entire amount served.
A reduction of the proportion of untouched salad portions could be achieved by making salad an item that needs to be ordered separately rather than it being automatically included on the standard tray with the main dish.
To reduce the waste of desserts, serving it in the afternoon to the patients in combination with the beverage round could have a positive effect. This would not lead to additional interruptions for the patients and it is perceived by the patients as an additional service.
Figure 5. Food waste components dinner
Error! Reference source not found. shows the food waste components for dinner. The main food waste components are, as was the case for lunch, dessert and salad. The portions are either eaten or not touched at all. As described for lunch, the amount of food waste for soup cannot be estimated and the components protein, vegetables and carbohydrates are mostly eaten. At one hospital the food waste amount for dinner is very low compared to the other two hospitals. It would be worthwhile investigating the reasons behind this. From a FM perspective, this fact has positive financial implications. However, it could also indicate that patients could be at risk of malnutrition.
Status of the trays at collection time
To learn more about the reasons behind the 15% trays returned untouched, it was informative to observe the status of the trays at collection time, as shown in Error! Reference source not found..
Figure 6. Status of the trays at collection time
Around 5% of the trays are returned untouched at lunch and dinner because patients are to be given nothing by mouth. In addition, 5% of the trays are returned untouched because patients had already been discharged. These are the main reasons besides the physical and mental condition of patients for the trays being untouched. In addition, a lack of communication as well as poorly working task and staff interfaces can be identified. For lunch around 10% and for dinner about 20% of patients want or need to eat later. Nearly 7% of the patients are not finished eating at lunch and at dinner when the trays get collected. These facts suggest that meal times may need to be reviewed. Overall, at breakfast 4% of the trays are returned untouched, for lunch it is almost 20% and for dinner a bit more than 10%. These trays are going through the whole process without fulfilling their purpose of feeding a patient.
Conclusions
The research project set out to explore the important parameters for the improvement of food service processes in Swiss hospitals, with a focus on whether examination of food waste could be used to identify these parameters. It was undertaken in the context of the new funding system for hospitals and focused on hospitals using the food provision system of cook & serve. The findings provide preliminary indications for FM managers of where resource optimisations regarding the parts of the food service associated with food waste can begin in order to improve service quality as well as to reduce waste and thereby to reduce costs. In addition, it provides the FM managers with additional arguments to give the responsibility of providing the food service process to one department.
Relevance of findings
Based on this research, the parameters influencing food waste in hospitals, when the plated food leaves the kitchen, when it is delivered to the patient and when it is returned to the dishwashing area as food waste, are identified, as shown in table three. They indicate where further process and cost optimisation is possible to improve service quality as well as to reduce costs. This is directly beneficial for the whole support processes in hospitals and consequently also for the FM industry. As there is almost no research done in this field, the findings are very relevant to the target group. Limitations of this study are that it was an exploratory study with focus on hospitals which use the cook and serve system. Additional research is needed to find out how these parameters can be identified in other hospitals with other food provision systems. Nevertheless, this research provides the basis for further research projects.
Outlook
As a next step, the relationships between the identified parameters should be examined. In addition, research should be extending to other food provision systems which are used in hospitals other than the cook & serve system already studied. All future research activities should be done with the aim to provide FM managers in hospitals with evidence to support the implementation of measures which ensure efficient and effective support services.
References
Almdal, T., Viggers, L., Beck, A. M., & Jensen, K. (2003). Food production and wastage in relation to nutritional intake in a general district hospital -wastage is not reduced by training the staff. Clinical Nutrition, 22(1), 47-51. doi: 10.1054/clnu.2002.0590
Barton, A. D., Beigg, C. L., MacDonald, I. A., & Allison, S. P. (2000). High food wastage and low nutritional intakes in hospital patients. Clinical Nutrition, 19(6), 445-449. doi: 10.1054/clnu.2000.0150
Bundesamt für Gesundheit BAG. (2013). Spitalstatistiken Spitalsuche. Retrieved July, 1, 2013, from http://www.bag.admin.ch/hospital/index.html?webgrab_path=aHR0cDovL3d3dy5iYWctY W53LmFkbWluLmNoL2t1di9zcGl0YWxzdGF0aXN0aWsvcG9ydGFsX2RlLnBocD9uY XZpZD1zcGl0YWxwZGZ0eXAmYW1wO3N0ZXA9MSZhbXA7dHlwPWsxMTI%3D&l ang=de
CEN. (2006). Facility Management – Part 1: Terms and definitions (Vol. EN 15221-1). Brussels: European Committee for Standardization.
Dupertuis, Y. M., Kossovsky, M. P., Kyle, U. G., Raguso, C. A., Genton, L., & Pichard, C. (2003). Food intake in 1707 hospitalised patients: a prospective comprehensive hospital survey. Clinical Nutrition, 22(2), 115-123. doi: http://dx.doi.org/10.1054/clnu.2002.0623
Edwards, J. S. A., & Nash, A. H. M. (1999). The nutritional implications of food wastage in hospital food service management. Nutrition & Food Science, 99(2), 89-98. doi: 10.1108/00346659910254394
Flick, U. (2010). An introduction to qualitative research: SAGE.
Hofer, S., Honegger, F., & Züger, G. (2013). A Method to Benchmark Swiss Hospital Catering. International Journal of Facility Management, 4(3).
Saunders, M. N. K., Lewis, P., & Thornhill, A. (2009). Research methods for business students. Harlow: Pearson Education Limited.
Sonnino, R., & McWilliam, S. (2011). Food waste, catering practices and public procurement: A case study of hospital food systems in Wales. Food Policy, 36(6), 823-829. doi: 10.1016/j.foodpol.2011.09.003
SwissDRG. (2013a). Informationen zu SwissDRG. Retrieved March, 11, 2013, from http://www.swissdrg.org/de/07_casemix_office/InformationenZuSwissDRG.asp?navid=8
SwissDRG. (2013b). Ziele SwissDRG. Retrieved March,11, 2013, from http://www.swissdrg.org/de/07_casemix_office/Ziele.asp?navid=9
von Eiff, W. (2012). Speisenversorgung im Krankenhaus: Marketing-und Kosteneffekte durch Prozess-und Qualitätsmanagement. Ernährungs Umschau, 2, 78 -88.
Williams, P., & Walton, K. (2011). Plate waste in hospitals and strategies for change. e-SPEN, the European e-Journal of Clinical Nutrition and Metabolism, 6(6), e235-e241. doi: http://dx.doi.org/10.1016/j.eclnm.2011.09.006
Want even more Content?
Since you’re already a user, you know that IFMA’s Knowledge Library offers all FM content in one place. But did you also know that by signing up via email to become a registered user, you can unlock even more resources?
Signing up via email for registered access within the Knowledge Library brings more content and functionality to your fingertips. Expect to grow your facility management knowledge, career and network faster than ever before.
Categories
Real Estate and Property Management